Amblyopia is poor vision in an eye that did not develop normal sight during early childhood. This condition, sometimes referred to as "lazy eye," can run in families. The main causes of amblyopia are strabismus, refractive errors, or cloudiness of the eye tissues.
Amblyopia affects about three out of every 100 people. The best time to correct it is during infancy or early childhood, because after the first nine years of life, the visual system is normally fully developed and usually cannot be changed. It is recommended that children have their eyes and vision monitored by their primary care physician at their well-child visits. If there is a family history of amblyopia, children should be screened by an eye doctor.
Strabismus, or misaligned eyes, is the most common cause of amblyopia. The eye that is misaligned is ignored by the brain and "turns off." A refractive error (meaning an eye is nearsighted, farsighted, or has astigmatism) is another cause of amblyopia. If one eye has a very different refractive error from the other eye, or if both eyes have a very strong refractive error, amblyopia can develop in the eye or eyes that are out of focus. The most severe form of amblyopia occurs when cloudiness of the eye tissues prevents any clear image from being processed. This can happen in conditions such as infantile or developmental cataracts.
Amblyopia is detected by finding a difference in vision between the two eyes or poor vision in both eyes. The eye doctor will also carefully examine the eyes to see if other eye conditions are causing decreased vision.
Amblyopia is treated by forcing the brain to use the affected eye or eyes. If refractive errors are present, they are corrected with eyeglasses or, less commonly, with contact lenses or refractive surgery. If a cataract or other cloudiness is present, surgery may be necessary to clear the line of sight. Strabismus may require surgery before, during, or after the amblyopia treatment. Patching or blurring the sound eye is then used to improve the vision by forcing the brain to recognize and process information from the affected eye or eyes.
Patching is the most common treatment method for amblyopia. There are adhesive patches that should be placed over the eye, or felt patches that can fit over glasses. Compliance is often an issue. In children over three years of age positive reinforcement can be very effective. In younger children distraction and restraints may be required. Peeking can be an issue. Parents should watch for loose edges or extreme head postures, which would allow a child to see around the patch.
Eye drops which blur vision in the better seeing eye are also useful inmild to moderate amblyopia. These drops cause prolonged dilation and children will need to protect their eyes from the sun with sunglasses.
Once maximum vision has been obtained, treatment often needs to be continued part time for months to years to maintain the recovered vision. The earlier the treatment is begun, the more successful it will be.
Childhood Reading Problems
When children have difficulty reading, parents often think poor vision is the problem. If a visit to pediatric eye doctor rules out any medical or vision problems, your child may have a learning disability.
A learning disability is a disparity between a person's ability and performance in a certain area. It has nothing to do with intelligence or IQ. A learning disability can make it difficult to succeed in school and, if untreated, can get worse, causing a child to lose self-confidence and interest in school.
Identifying the learning disability is the first step in treating it. Dyslexia, a reading disability that may involve reversing letters and words, is one of the many learning disorders that can affect reading.
Poor reading is not usually an eye problem; however many treatments have been tried and rarely prove helpful. Colored lenses, special diets or vitamins, jumping on trampolines, or walking on balance beams have been prescribed without much success. Over time, these methods have tended to fall out of favor.
Children with learning disabilities benefit from various educational programs, in or out of school. Parents also play a vital role. They can support their children by reading with them at home. Children with learning disabilities need to be encouraged to develop strengths and interests so they can fully develop their unique talents and abilities.
There are some medical and visual problems that if left uncorrected can affect a child's ability to see a clear and single image. If your child has one of these conditions, the disruption to their vision may significantly impact their reading abilities. It is very important to catch these problems sooner rather than later so that your child doesn't fall too far behind. Some of these conditions may be treated with glasses alone while others can be treated with a vision training program. Your pediatric eye doctor can recommend the most appropriate treatment if your child has one of these problems.
Children's Eye Safety
Accidents resulting in serious eye injury can happen to anyone, but are particularly common in children and young adults. More than 90% of all eye injuries can be prevented with appropriate supervision and protective eyewear.
Goggles and face protection can prevent injuries in sports like baseball, basketball, racket sports, and hockey. It is more difficult to protect against injuries in boxing, although thumb-less gloves help. As paintball and air soft guns are becoming more popular, more eye injuries are seen as children and parents often forget about the importance of safety goggles and face protection.
Children with vision loss in one eye should wear polycarbonate safety glasses at all times and should wear safety goggles for sports and other dangerous activities. Choose frames and lenses that meet the American National Standards Institute (ANSI) standard for safety (Z87.1).
Appropriate adult supervision is an essential part of preventing eye injuries. Children should never be allowed to play with fireworks or BB guns. Sharp and fast-moving objects such as darts, arrows, scissors, knives, and even pencils or pens can be dangerous. Special care should be taken when working around lawn mowers, which can throw rocks and debris, and when banging two pieces of metal together, which can dislodge small shards of metal. Chemicals such as toilet cleaners and drain openers are especially hazardous.
Minor injuries, such as a foreign body or an abrasion (scratch) on the cornea, can be treated in the office. Any foreign material will be removed from the eye, an antibiotic eye drop or ointment may be used, and an eye patch may be applied for comfort. However, more serious injuries, such as blood inside the eye (hyphema), a laceration (cut) of the eye, or rupture of the eye, may require surgery or hospitalization.
Chemicals that burn should be rinsed from the eye immediately. Chemical burns can cause severe damage, so eyes should be flushed immediately. If sterile solutions or eyewashes are readily available, use them to flush the affected eye. If not, flush the eye with liberal amounts of water from the nearest sink, shower, or hose for ten minutes. Be sure water is getting under both the upper and lower eyelids. After the eyes have been flushed for ten minutes, bring the child to the eye doctor or emergency room immediately. The ultimate visual outcome after a chemical burn depends on the severity of the injury, which cannot always be identified in the initial examination.
Congenital Cataracts
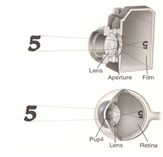
Your eye works a lot like a camera. Light rays focus through the lens on the retina, a layer of light-sensitive cells at the back of the eye. Similar to photographic film, the retina allows the image to be "seen" by the brain. A cataract is complete or partial opacification of lens material (nucleus, cortex, or capsule).
The loss of transparency may be so mild that vision is barely affected, or it can be so severe that no shapes or movements are seen--only light and dark. Eyeglasses or contact lenses can in some cases correct slight refractive errors caused by early cataracts, but they cannot sharpen your vision if a severe cataract is present.
Cataracts that occur in childten are different than cataracts which occur as an aging phenomenon in adults. As such they require a different evaluation, and different modalities of management, taking into consideration the different etiologies and the development of the visual system.In visually immature children, the age at onset and the degree of maturation of the visula system are additional considerations. The first six months of life are a period of critical visual development in infants. During this time, a clear focused retinal image is required to permit normal development of the visual system. If this is not present, either one or both eyes will not achieve it's fullpotential for viual acuity due to the development of irreversible deprivation amblyopia. The development of amblyopia continues to be a problem until maturity of the visual system is reached, roughly around the age of 8 years. Early diagnosis and prompt treatment are critical factors in determining the visual outcome in infants and children with cataracts.
There are many causes of congenital and childhood cataracts. Certain diseases, both metabolic and infectious, can cause the condition, and they can also be inherited in an autosomal dominant or recessive pattern. Cataracts can also be associated with specific genetic syndomes. However, in many cases, there is no identifiable cause.
A complete history and thorough eye exam can help establish the type and etiology of the cataract. In some cases laboratory testing and/or referrals to other specialists, such as genetists or rheumatologists, will be recommended.
Treatment for cataract in infants and varies depending on the nature of each patient's condition. Surgery is usually recommended very early in life, but many factors affect this decision, including the infant's health and whether there is a cataract in one or both eyes. If only one eye is affected by cataract, the infant's visual system can develop abnormally, and, if left untreated, serious vision problems and even vision loss can result. Therefore, removal is usually recommended within the first 4-8 weeks of life. In bilateral cases, surgery may be able to be delayed, however often the more effected eye is done first, followed 2-3 weeks later by the other eye.
Surgery in infants requires general anesthesia and is done in an operating room under sterile conditions. An incision is made in the cornea or sclera of the eye, and an opening is created in the anterior capsule allowing the removal of the lens nucleus and cortex using a specially designed aspiration-cutting instrument. In young children a part of the posterior capsule will also be removed to help prevent further opacification, often called a "secondary membrane". Even with removal of the posterior capsule, in some cases further laser or surgical intervention will be required.
Post operatively, a child will require a combination of antibiotic, steroid and dilating drops for several weeks. Your surgeon will give you explicit instructions. A shield will also be used to protect the eye, for about a week.
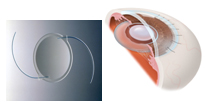
Usually, strong eyeglasses or contact lenses are prescribed for infants after surgery who are aphakic (without a lens). For babies over 6months of age, an artificial intraocular lens (IOL) may be recommended instead to replace the eye's natural lens.
The ophthalmologist can recommend which procedure and optical correction is best for your child. Many factors are involved in optical correction including focusing light on the retina, providing the ability to focus at both distance and near, protection from UV light, and the ability to change with a child's growth. Currently, there is no perfect method, and frequently a combination of intraocular lens or contact lens with glasses and a bifocal will be necessary.
After surgery, children must be followed closely, complications such as infection and retinal detachment are rare, but can be sight threatening when they occur. Glaucoma can occur at any time, and may require drops or further surgery, rates as high as 25% have been reported in eyes that have undergone cataract extraction. Strabismus (misalignment of the eyes) and amblyopia (weaker vision in one eye) are common in eyes that have cataracts, even once the lens has been removed. Occlusion therapy, such as patching, may be required until the child reaches visual maturity. The management of a child with cataracts requires a commitment from both the surgeon and the family, that extends from the timing of surgery to the lengthy rehabilition stage and beyond.
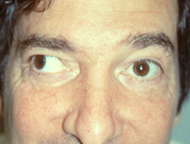
Esotropia
One common form of strabismus, or misaligned eyes, is called esotropia. Esotropia, or "crossed" eyes, occurs when the eyes turn inward towards the nose. Esotropia can be both infantile, when it occurs before six months of age, and accommodative, which is more likely to develop between six months and two and a half years of age.
Pseudostrabismus, or the false appearance of an eye turn, is often mistaken for true esotropia. In these children, the symmetry of the corneal light reflex can help to determine the alignment of their eyes. Infants often have wide, flat nasal bridges and prominent skin folds at the inner corner of their eyes, which give the appearance of crossing eyes.
With accommodative esotropia, when the child focuses the eyes to see clearly, the eyes turn inward. This "crossing" may occur when focusing at a distance, at close range, or both. These children typically have some degree of hyperopia or farsightedness. Eyeglasses reduce the focusing effort and often straighten the eyes. Sometimes bifocals are needed for close work. Sometimes children will not notice an improvement in their vision with their glasses. It is then important for parents to explain that the glasses are helping the child to use both eyes together and not to make objects look clearer. In a partly accommodative esotropia,significant crossing of the eyes persists with glasses and surgery may be required.
Young children withinfantile esotropia should first be checked for an accommodative component to the eye turn. If hyperopia is present, either glasses or phospholine iodide will be prescribed to reveal the amount of the eye turn that is due to focusing. Surgery is never performed to control the accommodative component. In most cases, early surgery, performed after six months of age, can align the eyes.
Esotropia is often treated by surgically adjusting the eye muscles under general anesthesia. The goal of surgery is to get the eyes close enough to perfectly straight so that it is hard to see any residual deviation and to allow binocular vision to develop.
The main sign of esotropia is an eye that is not straight. Sometimes children will squint one eye in bright sunlight or tilt their head in order to use their eyes together.
Amblyopia, or "lazy eye," is closely related to esotropia. Children learn to suppress the double vision associated with esotropia so effectively that the deviating eye gradually loses vision. It may be necessary to patch the good eye and have the child wear eyeglasses before treating the esotropia.
Estropia Left
Estropia Right
Pseudostrabismus
Exotropia
Exotropia is a misalignment of the eyes in which the eyes deviate outward. Though exotropia occurs less frequently than esotropia ("crossed eyes"), it is still a common form of strabismus. Exotropia may occur only when the child is daydreaming, tired, or sick. Parents often notice that the child squints one eye in bright sunlight.
Intermittent Exotropia is the most common exodeviation in childhood. It can occur at any age, but most frequently between the ages of two and four years of age. The size of the deviation, its frequency, and the child's ability to control the drifting are important factors in determining treatment. The doctor may ask you to quantitate the amount of drifting that you see at home.
Convergence Insufficiency occurs when the near deviation is greater than the distance deviation. These children may complain of difficulty with reading and near work, and become more symptomatic during times of stress (ex.final exams).
Amblyopia, or "lazy eye", may develop with exotropia, although it is less common than with esotropia, as the deviation is usually intermittent. Children learn to suppress the double vision associated with exotropia so effectively that the deviating eye gradually loses vision.
The treatment for exotropia may include glasses to improve visual acuity, as well as, "over minus" corrections to improve alignment. Patching may be required in cases of amblyopia, or a strong eye preference. Prisms are more commonly used in adult patients. Convergence exercises have also been shown to improve control. Surgery to adjust the eye muscles is often recommended in cases of constant and intermittent exotropia. The goal of surgery is to get the eyes as straight as possible so that no residual deviation is visible and binocular vision can develop.
Exotropia Left, Child
Exotropia Right, Adult
Ptosis
Ptosis (toe-sis) is a condition in which the upper eyelid falls to a position that is lower than normal. The drooping eyelid can cover part or all of the pupil and interfere with vision, resulting in amblyopia. Ptosis can affect one eye or both eyes.
Ptosis may be present at birth or develop later in life. If a droopy eyelid is present at birth or within the first year of life, the condition is called congenital ptosis. In most cases of moderate or severe congenital ptosis, surgery is required to tighten the eyelid muscles or suspend the eyelid from the brow so that the eyelid is not covering the line of sight. If the ptosis is severe, surgery may be recommended in infancy. Often surgery is delayed until a child is 3 or 4 years old.
Amblyopia, or "lazy eye," is decreased vision in one or both eyes caused by lack of use. This condition can occur with congenital ptosis. If amblyopia is present, treatment with patching, eyeglasses, or eyedrops may also be necessary. If left untreated, amblyopia may lead to permanent vision loss.In infants with congenital ptosis, patching the healthy eye may be used to helpprevent development of amblyopia in the eye with the droopy eyelid.
Tearing
Although it can be caused by wind, smoke, or pollen, an excess of tears in children is often caused by congenital nasolacrimal duct obstruction, a condition in which a baby's tear duct is blocked instead of draining normally through the duct into the nose. The condition can be recognized by tears that build up on the surface of the eye and overflow onto the eyelashes, eyelids, and down the cheek. Because the tears are not draining normally, babies will sometimes get infections, which can cause red, swollen eyelids and yellowish-green discharge.
Congenital nasolacrimal duct obstruction is usually caused by the failure of a thin tissue at the end of the tear duct to open properly when the child is born. It can also be caused by a lack of openings to the duct system at the eyelids, by infections, and by abnormal growth of the nasal bone, which pinches off the tear duct. Some infants may have excessive tearing due to narrow tear ducts rather than an obstruction. In this case, the tearing may be intermittent, occurring when the infant has a cold or during especially windy or cold weather. Finally, congenital glaucoma can cause tearing in children. This serious condition is often accompanied by other signs, including an enlarged eye, a cloudy cornea and light sensitivity.
Most babies born with blocked tear ducts do not need treatment. More than 90% of blocked tear ducts clear by themselves before the child turns 1 year old. If treatment is necessary, the first course of action is usually tear duct massage, along with topical antibiotics to treat infection. The tear sac is located between the inside corner of the eye and the side of the nose. The purpose of massage is to put pressure on the tear sac for a few seconds to pop open the membrane at the end of the tear duct. This is most easily done by putting your hands on each side of the baby's head and using your index fingers to press on the tear sac. This should be done several times a day, such as after feedings or diaper changes.
In certain circumstances, tear duct probing, balloon tear duct dilation, or tear duct probing with tube placement may be necessary. These procedures are performed under general anesthesia requiring a same day surgery at the hospital. Should your infant need treatment to remove a tear duct obstruction, ask your pediatric ophthalmologist to discuss appropriate treatment options with you.
Blinking
NORMAL BLINKING
Blinking is a physiologic response which involves relaxation of the levator muscle (which opens the eyelids) with simultaneous contraction of the palpebral portion of the orbicularis oculi muscles (which closes the eyelids).
Normal or spontaneous blink rates vary from twelve to twenty blinks per minute. The blink rate in infants is much lower and may normally be only one or two blinks per minute.
BLINKING IS A NORMAL FUNCTION THAT HELPS TO REMOVE FOREIGN MATERIAL
Blinking can be divided into spontaneous, reflex, and voluntary blinking. Heightened levels of awareness or increased anxiety may increase the blink rate whereas decreased spontaneous blink rates may result from anything that will depress the central nervous system.
Blinking helps to cleanse the cornea and anterior segment of the eye. Rapid phase cinematography has demonstrated that the blink closes the eyelids from their lateral most portions toward the nasal portion thus causing a squeegee effect pushing tears and foreign material toward the nasolacrimal collecting system, near the nasal insertion of the eyelids.
Blinking also serves to wet the cornea and redistribute the tear film over it. This serves to create an optically smooth interface between the corneal surface and the surrounding atmosphere.
DECREASED BLINKING
Decrease in spontaneous blinking may occur with central nervous depression, either drug related or when a patient is in a coma. It is also noted in some diseases of the central nervous system such as Parkinson's Disease.
Reflex blinking may also be decreased. Defects that reduce the sensation of the cornea, such as herpes keratitis or a congenital lack of sensation (Riley-Day Syndrome), may cause decreased intensity of afferent impulses or decreased stimulation for reflex blinking.
If the decreased corneal sensation is accompanied by other cranial nerve defects, the brain stem and the region of the cerebello-pontine angle, should be investigated.
Decreased intensity of strength of the blink may be caused by seventh cranial nerve dysfunction. This may be due to Bell's Palsy or to injury of the seventh cranial nerve. In either of these situations, the afferent or sensory pathway remains intact, but the efferent pathway to close the lids is abnormal. (The patient will usually have corneal sensation.)
EXCESSIVE BLINKING
Excessive blinking may be related to either increased duration of lid closure or it may be due to an increased rate of blinking. Prolonged lid closure may be related to blepharospasm (which is very uncommon in children), central nervous system stimulation, and tardive dyskinesia (a side effect of some tranquilizers). Increased blinking rate may be due to irritative lesions in the central nervous system (meningitis) or ocular abnormalities.
Some ocular abnormalities which are associated with increased blinking rate are: albinism, corneal dystrophy, achromatopsia, and any condition that may cause diffraction of light striking the cornea, such as a corneal abrasion or a corneal scratch caused by a foreign body lodged under the eyelid. An allergy may cause blinking with or without sensations of ocular irritation. The allergic blinking pattern can exhibit an increased frequency for lid closure and /or "rolling" of the eyes.
EXCESSIVE BLINKING IN CHILDREN IS FREQUENTLY DUE TO A NERVOUS TIC
Finally, the most common cause of excessive blinking is behavior abnormalities commonly referred to as tics. These habits usually last for 2 - 3 months or so and are not associated with ocular pathology. These common tic disorders are transient and usually last less than a year. These repetitive activities are self limited and are not associated with vocal or other complex involuntary activity. Tics may be accompanied by functional eyelid pulling, squinting, or rapid voluntary blinking.
TOURETTE SYNDROME
This rare syndrome will usually develop in childhood (mean age 7 years old) and is a life long disorder. In most families this will follow an autosomal dominant hereditary pattern of inheritance modified by environmental factors. This syndrome comprises multiple complex motor and / or vocal tics which occur concurrently.
EVALUATION
To evaluate the blinking, a complete history should be obtained. The drug history should include use of phenothiazines (antiemetics), since these may cause tar dive dyskinesia.
David Taylor, M.D. has outlined some helpful questions in his book "Pediatric Ophthalmology".
1. Is it the blink or is it the duration of the blink that is abnormal?
2. Does the blink occur at any specific situation, time of day, or in bright sunlight? What is its relation to stress or a particular social situation? Does the blink occur in the wind or when the child is attempting to look at something?
3. Is the eye or eyelid ever red or painful? Is the eyelid being irritated by a condition such as blepharitis?
4. Does the entire lid twitch or just a portion of the lid (myokymia)? Do other facial muscles also twitch (hemifacial spasm)? Are there accompanying eye movement disorders Are there eyelid disorders or any signs of central nervous disease?
5. Is there a history of behavioral or psychological problems?
6. What is the duration of symptoms? (Tourettes Syndrome should become a consideration when the blinking persists more than a year and is associated with other signs such as vocal tics and other complex movements.)
The physical exam should include a measurement of visual acuity to exclude large degrees of astigmatism or other undetected refractive errors.
The external eyelids should be examined. The lid margins and the bulbar and palpebral conjunctiva of the lower and upper lids should be inspected. When palpebral blinking is associated with allergy the conjunctiva is irritated or has a cobble stone appearance. When this is observed, the search for an irritant or an allergen should be investigated. This is best done by a review of exposure or activity earlier in the day or during the previous day. If there is suspicion of a foreign body, fluorescein stain of the cornea can be applied and a cobalt blue light can be used to detect any corneal surface irregularities. A careful search for a foreign body or eyelash in the cul de sac or on the cornea should be done in any patient with monocular blinking or squinting.
In older children, examination using a slit lamp may be helpful. The cornea should be checked for sensation prior to installation of any anesthetic drops.
Other systemic symptoms should be looked for. Are there signs or symptoms of a seizure disorder or a neurological problem? If it is possible, refraction and a cover test should be performed to test for refractive errors and to exclude strabismus.
Some forms of achromatopsia may be associated with blinking and blepharospasm. Color vision testing will help to diagnose this defect. Children with albinism will have increased ERG responses and although the diagnosis is obvious on external examination, this test may be performed in very select situations.
In most children, the examination will be normal and if it is, reassurance can be given to the parent. In such cases, the blinking is usually a self-limited problem, due to a tic. Blinking will last for several weeks or for a few months and will then disappear. Sometimes all that is necessary is to reassure the child (and parent) that the eye exam is normal. The child should be reassured that the tic will gradually subside following the exam. It is best not to be confrontational to the child, which is, telling him or her that there is no problem or that you shouldn't be doing this. Rather, give the child reassurance and let the child eliminate the blinking at his or her own volition. If there is an allergic component, elimination of the allergen or reducing the exposure to the allergen is suggested. IF THERE ARE SIGNS OF AN ALLERGY - TREATMENT IS INDICATED. Eye drops such as a topical antihistamine or Mast Cell Stabilizer may help. Use of mild topical corticosteroids four times a day may be helpful. Tics will increase with anxiety and if this is a component, a source of the problem may be looked for.
Brabec, Levin and Nelson have examined causes for functional blinking in childhood and found that new situations such as a new sibling, beginning reading in school, a new school situation, or a death in the family, were common problems that were associated with the onset of excessive blinking. Similar observations were made by Catalano, Trevisani and Simon when they investigated functional eyelid pulling in children. Further information on the differential diagnosis can be gained from Ellis's chapter in the book, Decision Making in Pediatric Ophthalmology edited by Gerhard Cibis, M.D.
Patching Tips
Adhesive patches come in multiple sizes and are available in most large chain pharmacies and may also be ordered on-line. Multi-color and design patches are available****Pirate patches or similar patches are not recommended since patients can peek around them****.
Felt EZ patches are an option, these are made for glasses.
If breakdown of skin occurs, stop patching for three days and then restart. It can be helpful to remove excess adhesive from the patch prior to placing it on the skin by touching the patch to clean clothing such as your pant leg before applying.
Do not place the patch on the glasses. Your child can easily peek around the patch if you do this.
Make sure that the patch is adherent to the skin so that no light gets under it. If the patient pulls away part of the patch and peeks, the patching is INEFFECTIVE.
If your child takes a nap, leave the patch on during this time. Try to avoid using more than one patch a day. The more you remove the patches the more skin breakdown occurs. Patching is effective only if your child is awake; therefore, patching time during sleep should not be added to the total number of hours patched.
Parents will choose the best time for their child to patch. If a child will patch during school that is fine. If the child is too embarrassed, do not force the issue. Instead, patch before and after school and increase patching during weekends and holidays.
Patching is like having a prescription for medication. IT IS IMPORTANT TO FOLLOW THE INSTRUCTIONS OF YOUR DOCTOR TO GET THE EXPECTED RESULTS.
The number of hours you patch is critical. If your child patches two hours in the morning followed by a two hour nap and the total prescribed patching time is six hours, four more hours of patching is needed. Patching the total number of hours at one time is the best regimen.
We realize that not every child will cooperate; try not to punish the child. Be as encouraging as possible. You can try to play games with the patch as well as participate in activities that distract the child. Sticker charts can also be effective as positive reinforcement.
We recommend an hour of detailed work such as handheld video games, puzzles or crafts while patching.
If you are really struggling with the adhesive patch, please talk to your doctor about alternative penalization treatment.
Stye Versus Chalazion
Definition. The eyelids can be the site of various lumps and bumps. Two common red elevations on the eyelids are a stye (hordeolum caused by a bacterial infection) and a chalazion (lipogranuloma from inflammation).
Anatomy. The eyelid can be divided into the lid margin which includes the eyelashes and the remainder of the eyelid. The lid margin is the area where the openings of several glandular ducts are found. The glands of Zeis and Moll are found near the eyelashes. When they are infected with bacteria, a stye develops.
The structural support of the eyelid is the tarsal plate, which is a flat, fibrous structure that contains the meibomian glands. These meibomian glands produce an oily material which exits from the small duct openings which are located along the eyelid margin near the eyelashes. The oily material helps to decrease tear evaporation and by surface tension, helps to spread the tears more evenly over the surface of the cornea. Pathophysiology. If the meibomian gland or duct becomes obstructed, the oily material creates an inflammatory reaction in the surrounding tissue. If this persists, the reaction will stimulate the formation of fibrous tissue around the inflammation. The initial obstruction of the gland or its duct may be unexplainable. There are, however, some predisposing factors for formation of the chalazion. These are bacterial infection, rubbing of the eyes, long-term infection of the eyelid margin with crusting and redness(blepharitis), or altered, thickened glandular secretions.
Initially, the involved area of the chalazion can be swollen and red. This either will resolve or form a lump in the eyelid between the eyelash area and the fold of the eyelid. If the chalazion is small, it may resolve and disappear. Others will become quiet, or stable, and remain as a smooth painless lump. On rare occasions, they will become larger and erupt through the skin of the eyelid or protrude from the inner surface of the eyelid. The latter type can cause a smooth, 2 to 4 millimeter pink-red mass of tissue which resembles a small mushroom or pancake on the underside of the lid.
An infectious stye may occur as a red, slightly tender, raised area on the anterior lid surface. This pustular area can enlarge and involve the entire eye lid and produce eyelid edema, ecchymosis or even cellulitis.
TREATMENT FOR STYE (HORDEOLUM)
Since a stye is an infection, it will usually respond to warm compresses and topical or systemic antibiotics. Cultures are difficult to obtain unless an actual pustule occurs. Most organisms will be gram positive unless the child's immune system is compromised. TREATMENT FOR A CHALAZIONMedical. Initial treatment consists of moist heat applied to the eyelid, 2 to 4 times a day. This is best achieved by resting a moist wash cloth against the closed eyelid. Depending upon the suspected ratio of infection to inflammation, an antibacterial ointment or antibacterial/steroid ointment may also be applied to the eyelid. In select patients with fair pigmentation, a steroid injection into the chalazion may produce resolution.
Surgical. If the chalazion does not respond in a few weeks to a month, excision of the chalazion is usually suggested. In young children and adolescents surgery is done in the operating room with the help of a brief anesthetic. This permits excision without the risk of injury due to an uncooperative child. Surgery is typically performed as an outpatient and patients are discharged shortly after full recovery from the anesthesia.
Technique. Whether the chalazion is presenting externally through the eyelid skin or internally from the inner surface of the eyelid, the contents of the chalazion and the surrounding fibrous sack are excised. This involves a cut in the eyelid either internally or in rare cases externally. When an external approach is used, the horizontal skin incision is closed with absorbable sutures. There is usually minimal or no scarring of the skin. When excised internally, the contents are removed through a vertical incision and sutures are not necessary. After the surgery is completed, an antibiotic ointment is placed on the eyelid skin or under the eyelids. A soft eye patch may be used for a few hours after surgery.
Post-Operative Care and Follow-Up. Ophthalmic ointment is used for the next 5 days. The child should refrain from swimming for one week. Other than this, there are no restrictions in activity. After 7 to 10 days, the patient's progress is checked. A chalazion will not return if the gland is removed. However, other glands may become involved in other areas in susceptible individuals.
Allergic Conjunctivitis
Allergy-related eye symptoms commonly occur at the beginning of summer. Patients will frequently complain about irritation of the eyes caused by tree and grass pollens and mold spores in the air.
In the fall, the irritant is usually pollen from ragweed. Theses antigens, in addition to affecting the nose and upper respiratory system, will also affect the mucous membranes of the eye. There are three types of conjunctivitis that have an allergic basis: Hay fever Conjunctivitis, Vernal Keratoconjunctivitis, and Giant Papillary Conjunctivitis. These are not the same as "pink eye" and are not contagious.
HAY FEVER CONJUNCTIVITIS
Hay fever conjunctivitis is another term used for seasonal conjunctivitis. This represents a Type I allergic reaction characterized by conjuntival hyperemia, redness and slight swelling of the conjuctiva. The cornea is typically not involved.
VERNAL KERATOCONJUNCTIVITIS
This form of keratoconjunctivitis is uncommon and usually occurs in black children. This is a recurrent bilateral inflammation of the conjunctiva with a periodic seasonal incidence. It is self-limited in character and consists of an inflammatory response on the underside of the tarsus of the eyelids. There may be some white benign, gelatinous masses near the peripheral cornea. This will give the junction of the cornea and sclera a "pearl" appearance. Commonly, there is light sensitivity, conjunctival injection, tearing, and a mucinous discharge containing eosinophils. Treatment, if severe, consists of steroid eye drops and mast cell stabilizers.
GIANT PAPILLARY CONJUNCTIVITIS
This is a form of allergy usually associated with a reaction on the underside of the eyelids to contact lenses, or more commonly, the solutions used to clean contact lenses. A giant papillary response on the everted surface of the upper eyelid occurs and will give the surface a "cobblestone" appearance. These giant bumps can sometimes scratch the surface of the eye, which can be painful. Severe forms of this reaction will preclude the patient's use of contact lenses.
SYMPTOMS OF ALLERGIC CONJUNCTIVITIS
Symptoms are most commonly experienced shortly after exposure of the eye to the inciting allergen. The most frequent symptom is itching. This may be accompanied by burning and production of a watery discharge. The symptoms may be mild and self-limited or the eye and secretions may become secondarily infected by the child rubbing the eye with a dirty hand. In this case, the symptoms may be more pronounced in the eye on the same side as the dominant hand. Children and adults will frequently rub their eyes, though this usually worsens the itching. The eyelids may be puffy and the conjuctiva may be congested. Initially, the discharge is watery, but if the exposure is chronic, the tears may become thick and mucus like. A secondary infection with bacteria may cause the discharge to become cloudy. The cornea is rarely involved in typical forms of hay fever conjunctivitis. If it is, mild light sensitivity may occur and this is usually due to the child's rubbing of his or her eye. Most cases are initially seen in children four to six years of age. The symptoms will usually return each year at a similar time.
SIGNS OF ALLERGIC CONJUNCTIVITIS
The signs and symptoms of seasonal allergies are rarely limited to the eyes. The above findings are usually accompanied by rhinitis, asthma or atopic dermatitis. The signs associated with allergic involvement of the eyes are puffiness and swelling of the skin of the upper and lower eyelids. This may be severe enough to cause closure of both eyes due to the swelling. On rare occasions, the conjunctiva will become glassy and will frequently exhibit chemosis, or a collection of fluid and protein under the conjunctival tissue.
This may have a striking appearance with rapid onset lasting for a period of an hour or two with resolution of findings or it may be more chronic. Findings may be severe enough to prompt a visit to your office or to an emergency facility after hours. Conjunctival vessels will become dilated and there may be papillary response on the underside of the lids involving the tarsal conjunctiva. This can be looked for if the lids are gently everted. Patients with limbal vernal conjunctivitis may have some succulent collections of eosinophils at the periphery of the cornea. Light sensitivity or photophobia is usually severe.
EVALUATION
Since mild forms of allergic conjunctivitis are self-limited, usually no specific allergy testing is necessary. A thorough history and review of the common allergic agents may be sufficient to minimize or eliminate the child's contact with the allergen, and therefore, control the symptoms. If the discharge is purulent, eye cultures may be recommended and a conjuctiva scrapping may be performed to look for eosinophils. If the symptoms are repetitive and severe, skin testing may be considered. If the allergen suspected is ragweed, RAST testing may be requested.
TREATMENT
The first treatment efforts for allergic conjunctivitis are to minimize or eliminate exposure to the allergen. Thorough washing of the hands and cool compresses applied around the eyes will reduce the irritation. This will frequently be all that is necessary to reduce symptoms and reduce the concentration of the allergen.
Mild Symptoms. Topical over-the-counter artificial tears may be helpful in mild cases. The use of these drops four times a day combined with cool compresses will usually relieve mild symptoms.
Mild to Moderate Symptoms. The prescription of a combination of antihistamine drops, in addition to the above measures, may be sufficient to control mild to moderate cases of allergic conjunctivitis. When secondary infection accompanies the allergic response, an antibiotic drop may be added to the treatment program.
Severe Allergic Responses. For the more refractory cases, a mild topical corticosteroid preparation should be considered. For more difficult cases, steroid eye drops may be more effective. Steroid eye drops have a risk of elevating intraocular pressure in patients who are "steroid responders". Although patients who respond to steroids are uncommon in our population, careful monitoring of the intraocular pressure should be performed when patients are on these agents for several weeks. Other side effects of these stronger preparations may occur. These include increased susceptibility to infection and reactivation of viral (herpetic) disease. After years of using a preparation, early cataractous changes may be observed.
If the patient can anticipate exposure to an allergen, prophylaxis with a Mast Cell Stabilizer eye drop may be helpful to control eye symptoms. It's use for two days prior to exposure will stabilize the cell membranes of MAST cells and decrease the severity of the Type I allergic response seen with hay fever conjunctivitis. This type of medication is also good for treating giant papillary conjunctivitis and limbal vernal keratoconjunctivitis. The response to Mast Cell Stabilizers is not immediate and medication must be continued for lasting effect.
The goal of a treatment plan is to control the signs and symptoms throughout the season and to minimize any conjunctival changes resulting from the allergic reaction. Mild allergic symptoms usually do not cause permanent changes or lasting effects on the eye and its surrounding structures.
Children & Vision
Many people are confused about the importance of eyeglasses for children. Learn the truths and myths here.
Pediatric Eye Doctors Cranberry Pittsburgh Opthalmology Stabismus Adult Kids Doctor Adult Eye Pedatric Pediatric Opthamology Eyedoctor eye doctor pittsburgh Pittsburgh Eye Pediatric Ophthalmology Pediatric Eye Doctor Doctor Strabismus Pittsburgh Strabismus Pitsburg Pittsburg Pitsburgh Eye Doctor Kids Childrens Eye Doctor Pittsburgh Childrens Cranberry Mars Wexford Butler North Hills Pennsylvania Pittsburgh Pa Pediatric Eyes Examine Kid Kids Eye Doctor Jane Hughes MD Joseph Paviglianiti MD Eric Pennock MD Michelle Wertelet OD Eye Surgery Surgery Pediatrics Pittsburgh Kids Eye Doctor Eye Doctors Cranberry Pittsburgh Opthalmology Stabismus Adult Kids Doctor Adult Eye Pedatric Pediatric Opthamology Eyedoctor eye doctor pittsburgh Pittsburgh Eye Pediatric Ophthalmology Pediatric Eye Doctor Doctor Strabismus Pittsburgh Strabismus Pitsburg Pittsburg Pitsburgh Eye Doctor Kids Childrens Eye Doctor Pittsburgh Childrens Cranberry Mars Wexford Butler North Hills Pennsylvania Pittsburgh Pa Pediatric Eyes Examine Kid Kids Eye Doctor Jane Hughes MD Joseph Paviglianiti MD Eric Pennock MD Michelle Wertelet OD Eye Surgery Surgery Pediatrics Pittsburgh Kids Eye Doctor Eye Doctors Cranberry Pittsburgh Opthalmology Stabismus Adult Kids Doctor Adult Eye Pedatric Pediatric Opthamology Eyedoctor eye doctor pittsburgh Pittsburgh Eye Pediatric Ophthalmology Pediatric Eye Doctor Doctor Strabismus Pittsburgh Strabismus Pitsburg Pittsburg Pitsburgh Eye Doctor Kids Childrens Eye Doctor Pittsburgh Childrens Cranberry Mars Wexford Butler North Hills Pennsylvania Pittsburgh Pa Pediatric Eyes Examine Kid Kids Eye Doctor Jane Hughes MD Joseph Paviglianiti MD Eric Pennock MD Michelle Wertelet OD Eye Surgery Surgery Pediatrics Pittsburgh Kids Eye Doctor Eye Doctors Cranberry Pittsburgh Opthalmology Stabismus Adult Kids Doctor Adult Eye Pedatric Pediatric Opthamology Eyedoctor eye doctor pittsburgh Pittsburgh Eye Pediatric Ophthalmology Pediatric Eye Doctor Doctor Strabismus Pittsburgh Strabismus Pitsburg Pittsburg Pitsburgh Eye Doctor Kids Childrens Eye Doctor Pittsburgh Childrens Cranberry Mars Wexford Butler North Hills Pennsylvania Pittsburgh Pa Pediatric Eyes Examine Kid Kids Eye Doctor Jane Hughes MD Joseph Paviglianiti MD Eric Pennock MD Michelle Wertelet OD Eye Surgery Surgery Pediatrics Pittsburgh Kids Eye Doctor Eye Doctors Cranberry Pittsburgh Opthalmology Stabismus Adult Kids Doctor Adult Eye Pedatric Pediatric Opthamology Eyedoctor eye doctor pittsburgh Pittsburgh Eye Pediatric Ophthalmology Pediatric Eye Doctor Doctor Strabismus Pittsburgh Strabismus Pitsburg Pittsburg Pitsburgh Eye Doctor Kids Childrens Eye Doctor Pittsburgh Childrens Cranberry Mars Wexford Butler North Hills Pennsylvania Pittsburgh Pa Pediatric Eyes Examine Kid Kids Eye Doctor Jane Hughes MD Joseph Paviglianiti MD Eric Pennock MD Michelle Wertelet OD Eye Surgery Surgery Pediatrics Pittsburgh Kids Eye Doctor Eye Doctors Cranberry Pittsburgh Opthalmology Stabismus Adult Kids Doctor Adult Eye Pedatric Pediatric Opthamology Eyedoctor eye doctor pittsburgh Pittsburgh Eye Pediatric Ophthalmology Pediatric Eye Doctor Doctor Strabismus Pittsburgh Strabismus Pitsburg Pittsburg Pitsburgh Eye Doctor Kids Childrens Eye Doctor Pittsburgh Childrens Cranberry Mars Wexford Butler North Hills Pennsylvania Pittsburgh Pa Pediatric Eyes Examine Kid Kids Eye Doctor Jane Hughes MD Joseph Paviglianiti MD Eric Pennock MD Michelle Wertelet OD Eye Surgery Surgery Pediatrics Pittsburgh Kids Eye Doctor Eye Doctors Cranberry Pittsburgh Opthalmology Stabismus Adult Kids Doctor Adult Eye Pedatric Pediatric Opthamology Eyedoctor eye doctor pittsburgh Pittsburgh Eye Pediatric Ophthalmology Pediatric Eye Doctor Doctor Strabismus Pittsburgh Strabismus Pitsburg Pittsburg Pitsburgh Eye Doctor Kids Childrens Eye Doctor Pittsburgh Childrens Cranberry Mars Wexford Butler North Hills Pennsylvania Pittsburgh Pa Pediatric Eyes Examine Kid Kids Eye Doctor Jane Hughes MD Joseph Paviglianiti MD Eric Pennock MD Michelle Wertelet OD Eye Surgery Surgery Pediatrics Pittsburgh Custom Website Design